
Summary
Sarcopenia represents one of the largest remaining untapped pharmaceutical markets. Defined by the progressive loss of skeletal muscle mass, strength, and physical performance with aging or chronic disease, it affects tens of millions of adults worldwide and drives enormous healthcare costs through falls, frailty, loss of independence, and increased mortality. However, despite this burden, no drug has yet been approved specifically for its treatment or prevention.
The development landscape is characterized by an open market with minimal direct competition in the regenerative oral space. Regulatory pathways are still being defined, with recent FDA interactions and workshops emphasising the need for clinically meaningful improvements in physical function and patient-reported outcomes rather than surrogate measures such as muscle mass alone. While this creates a significant hurdle for purely protective or anabolic interventions, it offers a clear first-mover advantage for agents that can successfully demonstrate functional benefit through adaptive repair.
For a differentiated regenerative approach, the opportunity extends well beyond primary sarcopenia into adjacent indications such as osteosarcopenia, frailty, muscle preservation during GLP-1 agonist therapy for obesity, and secondary sarcopenia in chronic degenerative diseases. The reward for the right agent is substantial: the potential to establish a new therapeutic category with blockbuster potential while delivering meaningful improvements in healthspan and quality of life for a rapidly growing patient population.
Indication and unmet need
Sarcopenia is formally recognized in the International Classification of Diseases (ICD-10-CM code M62.84)1. Diagnostic criteria, most commonly those from the European Working Group on Sarcopenia in Older People (EWGSOP2), require evidence of low muscle strength, with low muscle quantity or quality, and often low physical performance.2 Two main forms are recognized: primary sarcopenia, driven primarily by aging, and secondary sarcopenia, which occurs in the context of chronic disease, immobility, or medication.3
Prevalence rises sharply with age: estimates suggest that up to 16% of the elderly are affected worldwide, the number rising to 50% amongst those aged over 80.4,5 Onset of muscle loss can begin as early as 30 years6. Secondary sarcopenia is common in conditions such as rheumatoid arthritis, heart failure, COPD, cancer, and chronic kidney disease4. The clinical consequences are profound. Sarcopenia is a major contributor to falls and fractures, loss of mobility and independence, prolonged hospital stays, and increased mortality. It amplifies the burden of other age-related conditions and is a core component of frailty.2 Economically, the direct and indirect costs are enormous, estimated at >$18 bn p.a. in direct US healthcare costs7, and >$40 bn pa when falls, nursing home admissions, and lost productivity are included.8
Current management is almost entirely non-pharmacological: resistance exercise, protein supplementation, and management of underlying conditions2. While effective when implemented, adherence is poor, access is limited, and benefits are often modest or not sustained. There is therefore a clear and urgent need for pharmacological interventions that can enhance or complement lifestyle measures.9
No drug is currently approved anywhere in the world specifically for sarcopenia. This creates a rare situation in modern pharmaceutical development- a genuinely open market. Existing off-label approaches (e.g., testosterone in men, certain nutritional supplements) have limited efficacy, narrow applicability, or unfavourable safety profiles for long-term use in older adults. A new therapy therefore has the chance to establish a new, first-in-class paradigm going beyond symptomatic or purely anabolic approaches by offering improved muscle function, reduced fall risk, preserved independence, and better quality of life.
Competitive pipeline
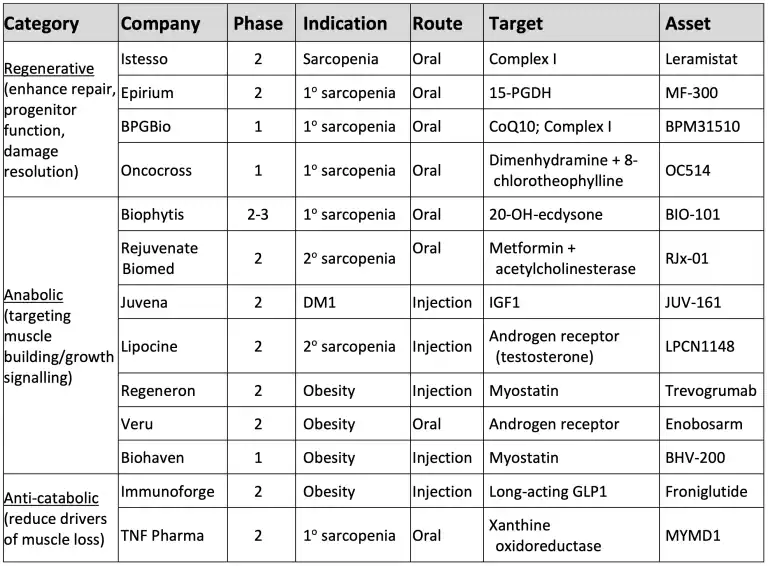
The sarcopenia development landscape is shown in Figure 1 and the pipeline in Table 1.
The sarcopenia pipeline is active but remains early to mid-stage with no agent approved or definitively positioned for broad primary sarcopenia approval. The pipeline shows healthy diversity: strong representation in anabolic (androgen/myostatin/IGF-1 axes, which have the most direct mass-building precedent), emerging anti-catabolic options targeting inflammaging or muscle cell death, and innovative regenerative approaches leveraging mitochondrial modulation, PGE2 signaling, progenitor proliferation, and endogenous repair.
The most advanced candidate is Biophytis’ BIO101 (Sarconeos), an oral mas receptor agonist that has received authorization to initiate a Phase 3 program (SARA-31). Other notable programs include MYMD-1 (an oral TNF-α inhibitor), Epirium’s MF-300 (oral 15-PGDH inhibitor), and Lipocine’s LPCN 1148 (oral testosterone prodrug) which has a Fast Track designation in cirrhosis-related sarcopenia.
A larger number of myostatin/activin pathway inhibitors (mostly injectable monoclonal antibodies such as bimagrumab and trevogrumab) are in development, but these are increasingly focused on muscle preservation in the context of obesity treatment with GLP-1 agonists rather than primary sarcopenia. This creates a natural segmentation: anabolic or anti-catabolic injectables for specific secondary indications versus agents targeting broader age-related or degenerative muscle loss.
Figure 1: Sarcopenia development landscape
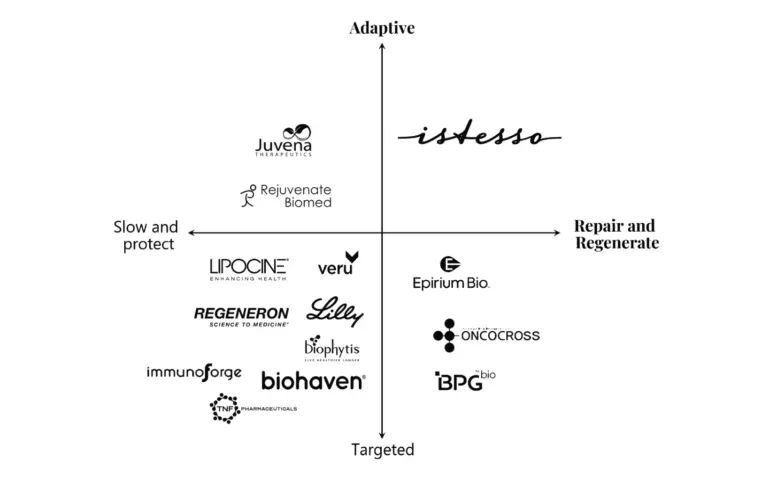
Table 1 Sarcopenia pipeline overview
Critically, there is minimal pipeline competition in the regenerative oral space, i.e. for agents that aim to enhance endogenous repair and regeneration of muscle rather than purely stimulating anabolism or blocking catabolism, and even less so in agents that can elicit an adaptive repair phenotype. This differentiation is significant. Precedent indicates that purely anti-catabolic approaches show a minimal functional benefit, while anabolic approaches primarily increase muscle mass or volume with inconsistent translation to function.10, 11 Those approaches with a regenerative component include:
- Istesso (Leramistat, Mitochondrial Complex I modulator, Phase2 primary and secondary sarcopenia): leramistat elicits an adaptive repair response, not only protecting muscle mass and restoring and improving muscle function, but also integrating benefits across multiple axes across both primary and secondary sarcopenia.
- Epirium Bio (MF-300, 15-PGDH inhibitor, oral, Phase 2, primary sarcopenia): MF300 inhibits 15-hydroxyprostaglandin dehydrogenase, elevating PGE2 levels to control inflammation, increase progenitor function and accelerate recovery of muscle force after nerve injury and restore muscle strength and quality without necessarily increasing overall mass.12
- Juvena Therapeutics (JUV-161, IGF1, injection, Phase 2, DM1 with muscle involvement). IGF-1 is a canonical anabolic factor that activates PI3K/Akt/mTOR signaling to drive protein synthesis, hypertrophy, and myoblast differentiation13. It also activates muscle satellite cells, such that this agent also shows regenerative potential.14 The primary intent in the lead indication (myotonic dystrophy type 1) is to counteract atrophy through growth promotion.
- Oncocross (OC514, dimenhydrinate repurposed formulation [diphenhydramine + 8-chlorotheophylline], oral, Phase 1, sarcopenia): Dimenhydrinate promotes muscle progenitor cell proliferation and myotube formation to elicit muscle tissue regeneration in models of chemotherapy-induced sarcopenia and DMD.15
Market Opportunity and Size
Current market size estimates for sarcopenia treatments range from approximately USD 1.5–3.2 billion in 2025, with projections reaching USD 5–5.6 billion by 2030–2034 (CAGRs of 5.7–10.6%).16,17,18,19 These figures largely reflect anticipated uptake of pipeline candidates in a market that does not yet exist in any meaningful commercial sense. The true addressable market, should an effective and well-tolerated therapy emerge, is substantially larger.
Sarcopenia affects a large and growing population in aging societies (see Appendix 2). Even modest penetration in key markets (United States, Europe, Japan) at premium pricing justified by meaningful functional benefit and healthcare cost offsets (reduced falls, hospitalizations, and institutional care) could support multi-billion-dollar peak sales. Adjacent indications such as osteosarcopenia20, frailty21, muscle preservation during obesity therapy22, and secondary sarcopenia in chronic disease could further expand the opportunity. Thus, a successful agent could realistically target peak sales in the range of several billion dollars annually, placing it among the largest pharmaceutical markets if the category is successfully established.
The economic case is compelling for payers as well as patients. Effective sarcopenia therapy has the potential to reduce the substantial downstream costs associated with falls, fractures, loss of independence, and prolonged hospital stays.8 Demonstrating these outcomes in clinical development will be critical for favorable reimbursement and broad access.
Key Hurdles and Risks
Several hurdles need to be overcome to successfully launch and commercialise a product in this emerging space.
The primary risk remains the lack of formally guided and validated pivotal endpoints accepted by regulators. At present there is no established surrogate that reliably predicts clinical benefit in either primary or secondary sarcopenia. Muscle mass or strength improvements alone have historically been viewed as insufficient without demonstration of functional or patient-centered outcomes. Recent FDA engagement, including the December 2024 SCWD Regulatory Workshop23, has provided some directional guidance in this regard. The agency has emphasized that approval will likely require evidence of clinically meaningful improvement in how patients function or feel, typically measured by validated physical performance tests (Short Physical Performance Battery [SPPB], habitual gait speed, stair-climb test, or 6-minute walk test) and/or patient-reported outcomes.24
This creates both challenge and opportunity. The absence of a fully precedent pathway means sponsors must engage early and proactively with FDA to align on endpoint strategy, population definition, and evidence requirements. For a regenerative agent capable of demonstrating both structural repair signals and functional improvement, there is the potential to help shape the regulatory framework itself, establishing new benchmarks for what constitutes meaningful benefit in sarcopenia and related conditions.
Patient heterogeneity poses a second key challenge. Sarcopenia populations are diverse (primary vs. secondary, varying severity, comorbidities)4 and, therefore, enrichment strategies and clear subpopulation definition will be essential to demonstrate robust signals. This is complicated by the specialised nature of conducting studies in older adults, who are often frail and present with multiple comorbidities.
Finally, several commercial risks will present for a successful product. These include reimbursement uncertainty in a new indication, pricing pressure in elderly populations, and the need to demonstrate not only efficacy but also clear healthcare economic value. Slow initial uptake is possible if the functional benefit, while clinically meaningful, is modest in magnitude. Thus, development of an appropriate path-to-market to both accelerate development, command appropriate pricing and reimbursement and enable expansion is critical.
Expansion to Adjacent Indications
A successful sarcopenia therapy, particularly one with a regenerative, repair-enhancing mechanism, has natural expansion opportunities into several high-value adjacent areas:
Osteosarcopenia and osteoporosis: The close interplay between muscle and bone makes dual benefit highly attractive. Agents demonstrating effects on both could command premium positioning and broader labelling.
Frailty and healthy aging: Prevention or delay of frailty in at-risk older adults represents a large preventive opportunity, potentially supported by health economic arguments around compression of morbidity.
Muscle preservation during GLP-1 agonist therapy: The rapid growth of incretin-based obesity treatments has created intense interest in agents that can mitigate muscle loss. An oral regenerative approach could be positioned as complementary or combination therapy.
Secondary sarcopenia in chronic disease: RA, heart failure, COPD, cancer cachexia, and chronic kidney disease all feature muscle wasting that could benefit from repair-enhancing mechanisms. These indications may offer faster paths to approval in some cases and provide valuable label expansion.
A platform approach in which evidence is developed across primary and secondary sarcopenia while building toward broader musculoskeletal repair or healthy aging claims maximizes long-term value and creates multiple shots on goal.
Strategic Implications and Reward for the Right Agent
For a differentiated regenerative oral therapy, the strategic implications are highly favorable. The combination of an open market, limited competition in the adaptive repair/regenerative oral segment, and a mechanism aligned with evolving understanding of muscle biology creates a compelling opportunity to establish category leadership.
A safe, convenient agent that demonstrates both structural repair and meaningful functional improvement could achieve several transformative outcomes:
- Become the first approved therapy in a major new indication, setting the standard of care.
- Command premium pricing justified by functional benefit and cost offsets (falls reduction, independence preservation).
- Enable rapid expansion into multiple adjacent high-value indications, creating a platform franchise.
- Generate peak sales in the multi-billion-dollar range, representing one of the largest commercial opportunities in aging-related medicine.
Beyond commercial reward, there is substantial societal and scientific value. Successfully developing a sarcopenia therapy would validate a new therapeutic paradigm (regenerative repair rather than pure suppression or anabolism), improve healthspan for millions, and reduce the societal burden of frailty and loss of independence in aging populations. In this regard, the combination of scientific differentiation, strategic positioning, and unmet need makes sarcopenia one of the most attractive remaining opportunities in pharmaceutical development.
Conclusion
The absence of approved therapies, the clarity emerging from recent regulatory dialogue, and the growing recognition of its clinical and economic burden create the conditions for breakthrough progress in sarcopenia. While hurdles remain, particularly around endpoint definition, population heterogeneity, and demonstration of meaningful functional benefit, these are addressable with thoughtful trial design, early regulatory engagement, and a differentiated mechanism. The reward for the right agent is high, going beyond incremental market share to define a new category of musculoskeletal medicine. A company that can successfully navigate this landscape will deliver transformative benefit to patients while capturing one of the largest remaining pharmaceutical opportunities of the coming decade.

References
1 Anker SD, Morley JE, von Haehling S. Welcome to the ICD-10 code for sarcopenia. J Cachexia Sarcopenia Muscle. 2016 Dec;7(5):512-514. doi: 10.1002/jcsm.12147. Epub 2016 Oct 17. PMID: 27891296; PMCID: PMC5114626.
2 Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M; Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019 Jan 1;48(1):16-31. doi: 10.1093/ageing/afy169. Erratum in: Age Ageing. 2019 Jul 1;48(4):601. doi: 10.1093/ageing/afz046. PMID: 30312372; PMCID: PMC6322506.
3 Santilli V, Bernetti A, Mangone M, Paoloni M. Clinical definition of sarcopenia. Clin Cases Miner Bone Metab. 2014 Sep;11(3):177-80. PMID: 25568649; PMCID: PMC4269139.
4 Yuan H, Larsson SC. Epidemiology of sarcopenia: Prevalence, risk factors, and consequences. Metabolism, July 2023, 144: 155533,https://doi.org/10.1016/j.metabol.2023.155533.
5 von Haehling S, Morley JE, Anker SD. An overview of sarcopenia: facts and numbers on prevalence and clinical impact. J Cachexia Sarcopenia Muscle. 2010 Dec;1(2):129-133. doi: 10.1007/s13539-010-0014-2. Epub 2010 Dec 17. PMID: 21475695; PMCID: PMC3060646.
6 Walston JD. Sarcopenia in older adults. Curr Opin Rheumatol. 2012 Nov;24(6):623-7. doi: 10.1097/BOR.0b013e328358d59b. PMID: 22955023; PMCID: PMC4066461.
7 Janssen I, Shepard DS, Katzmarzyk PT, Roubenoff R. The healthcare costs of sarcopenia in the United States. J Am Geriatr Soc. 2004 Jan;52(1):80-5. doi: 10.1111/j.1532-5415.2004.52014.x. PMID: 14687319.
8 Goates S, Du K, Arensberg MB, Gaillard T, Guralnik J, Pereira SL. Economic Impact of Hospitalizations in US Adults with Sarcopenia. J Frailty Aging. 2019;8(2):93-99. doi: 10.14283/jfa.2019.10. PMID: 30997923; PMCID: PMC12275775.
9 Tarantino G, Sinatti G, Citro V, Santini SJ, Balsano C. Sarcopenia, a condition shared by various diseases: can we alleviate or delay the progression? Intern Emerg Med. 2023 Oct;18(7):1887-1895. doi: 10.1007/s11739-023-03339-z. Epub 2023 Jul 25. PMID: 37490203; PMCID: PMC10543607.
10 Mansoor, M. A. M., Alam, M. T., Lijeron-Herrera, F., & Masternak, M. M. (2026). Sarcopenia: Current practices and the challenge of translating pharmacological interventions into functional benefit. Advances in Translational Research, 1(1), 65-74. https://doi.org/10.1556/1661.2026.00109
11 Tu S, Hao X, Xu S, Jin X, Liao W, Xia H, Wang S, Sun G. Sarcopenia: Current Insights into Molecular Mechanisms, Diagnostics, and Emerging Interventional Approaches. Int J Mol Sci. 2025 Jul 14;26(14):6740. doi: 10.3390/ijms26146740. PMID: 40724988; PMCID: PMC12295260.
12 Webster M, Martin J, Fahr B, Khairallah R. MF-300 (15-PGDH enzyme inhibitor) reverses age-related muscle weakness in mice by restoring muscle quality. Innov Aging. 2024 Dec 31;8(Suppl 1):1145. doi: 10.1093/geroni/igae098.3672. PMCID: PMC11693172.
13 Yoshida T, Delafontaine P. Mechanisms of IGF-1-Mediated Regulation of Skeletal Muscle Hypertrophy and Atrophy. Cells. 2020 Aug 26;9(9):1970. doi: 10.3390/cells9091970. PMID: 32858949; PMCID: PMC7564605.
14 Okino, R., Mukai, K., Oguri, S. et al. IGF-I concentration determines cell fate by converting signaling dynamics as a bifurcation parameter in L6 myoblasts. Sci Rep 14, 20699 (2024). https://doi.org/10.1038/s41598-024-71739-y
15 Lee MH, Lee B, Park SE, Yang GE, Cheon S, Lee DH, Kang S, Sun YJ, Kim Y, Jung DS, Kim W, Kang J, Kim YR, Choi JW. Transcriptome-based deep learning analysis identifies drug candidates targeting protein synthesis and autophagy for the treatment of muscle wasting disorder. Exp Mol Med. 2024 Apr;56(4):904-921. doi: 10.1038/s12276-024-01189-z. Epub 2024 Apr 1. PMID: 38556548; PMCID: PMC11059359.
16 https://www.researchandmarkets.com/report/sarcopenia-drug
17 https://www.datamintelligence.com/research-report/sarcopenia-treatment-market
18 https://www.delveinsight.com/report-store/sarcopenia-market
19 https://www.sphericalinsights.com/reports/sarcopenia-treatment-market
20 Kirk B, Zanker J, Duque G. Osteosarcopenia: epidemiology, diagnosis, and treatment-facts and numbers. J Cachexia Sarcopenia Muscle. 2020 Jun;11(3):609-618. doi: 10.1002/jcsm.12567. Epub 2020 Mar 22. PMID: 32202056; PMCID: PMC7296259. 21 Martin FC, Ranhoff AH. Frailty and Sarcopenia. 2020 Aug
21 In: Falaschi P, Marsh D, editors. Orthogeriatrics: The Management of Older Patients with Fragility Fractures [Internet]. 2nd edition. Cham (CH): Springer; 2021. Chapter 4. Available from: https://www.ncbi.nlm.nih.gov/books/NBK565582/ doi: 10.1007/978-3-030-48126-1_4
22 von Haehling S, Sato R, Langer H, Khan MS, Coats AJS, Evans W, Heymsfield S, Anker SD. Muscle Loss in Obesity Therapy as a Therapeutic Target: Trial Design and Endpoints for Regulatory Discussions. J Cachexia Sarcopenia Muscle. 2025 Dec;16(6):e70147. doi: 10.1002/jcsm.70147. PMID: 41362110; PMCID: PMC12686571.
23 von Haehling, S., Langer, H., Heymsfield, S., Evans, W. and Anker, S. (2025), Sarcopenia in Ageing and Chronic Illness: Trial Endpoints and Regulatory Issues. Journal of Cachexia, Sarcopenia and Muscle, 16: e13841. https://doi.org/10.1002/jcsm.13841
24 https://www.fda.gov/files/about%20fda/published/The-Voice-of-the-Patient–Sarcopenia.pdf


